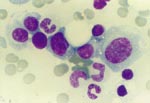
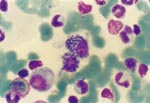
Hemolytic anemia, Leishmania donovani infection, bone marrow plasmatocytosis
Α 58 year-old Greek male was admitted to our Department because
of fever, pancytopenia and splenomegaly. Fever, up to 38.5 °C,
started fifteen days ago, during the evening. There were no chilling
or other symptoms. The administration of amoxycillin for five
days had no benefit. Fever continued for the whole day and fatigue,
weakness and dyspnea on slight exertion were added. Clarithromycin
and cefuroxime were administered for another six days with no
effect and the patient was admitted to the hospital. |