|
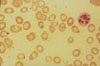
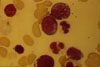
Toxic action of alcohol; folic acid deficiency, megaloblastic anemia; secondary sideroblastic anemia A 72 year old man presented at the Outpatient Clinic because of anemia. His past medical history included peripheral neuropathy detected a few years previously and chronic alcoholism. Physical examination revealed mild hepatosplenomegaly and multiple hepatic spiders. The blood count revealed mild normochromic macrocytic anemia (hemoglobin 6.9 g/dL, hematocrit 21%, reticulocytes 0.2%), leukopenia (WBC 3,200/μL with 45% neutrophils and a large proportion of hypersegmented cells) and mild thrombocytopenia. The LDH was 1850 U/L, bilirubin 1.20 mg/dL (conjugated 0.6 mg/dL), SGOT 101 U/L, SGPT 115 U/L, alkaline phosphatase 100 U/L, γ-GT 56 U/L, serum iron 105 μg/dL, serun ferritine 100 μg/dL, serum vitamin B12 328 ng/dL and serum folic acid <2.3 mg/dL. Bone marrow aspiration revealed erythroid hyperplasia with megaloblastoid proerythroblasts containing cytoplasmic vacuoles and a mild shift of the myeloid series to the left at the myelocyte stage. Prussian blue staining revealed normoblasts with augmentation of mitochondrial iron. Treatment with folic acid and pyridoxine led to an increase in the hematocrit one month after the initiation of therapy. |